Weak Muscles Form Weak Joints: The Biomechanical Reality
We have a saying in orthopedics and physiotherapy: " The muscle protects the bone."
When patients come to us with osteoarthritis (OA) of the knee or hip, they often blame "wear and tear." They believe they have "used up" their cartilage. But evidence suggests a different narrative.
Joints are designed to last a lifetime, provided they are supported by shock absorbers. Your muscles are those shock absorbers.
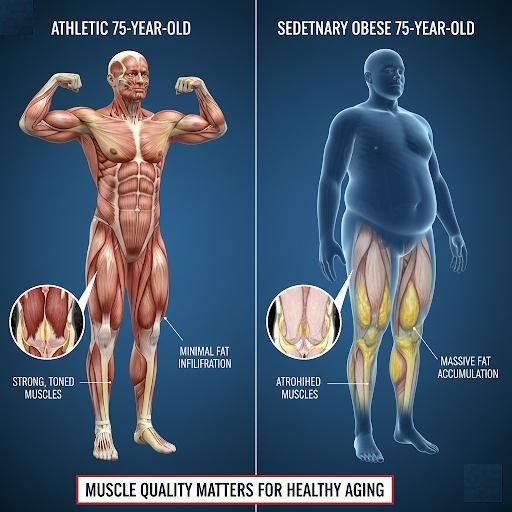
The Shock Absorber Effect: Every time you take a step, a force of 1.5 to 3 times your body weight travels up your leg. In a healthy leg (like our triathlete’s), the quadriceps eccentrically contract to absorb that force, dampening the load before it hits the joint surface.
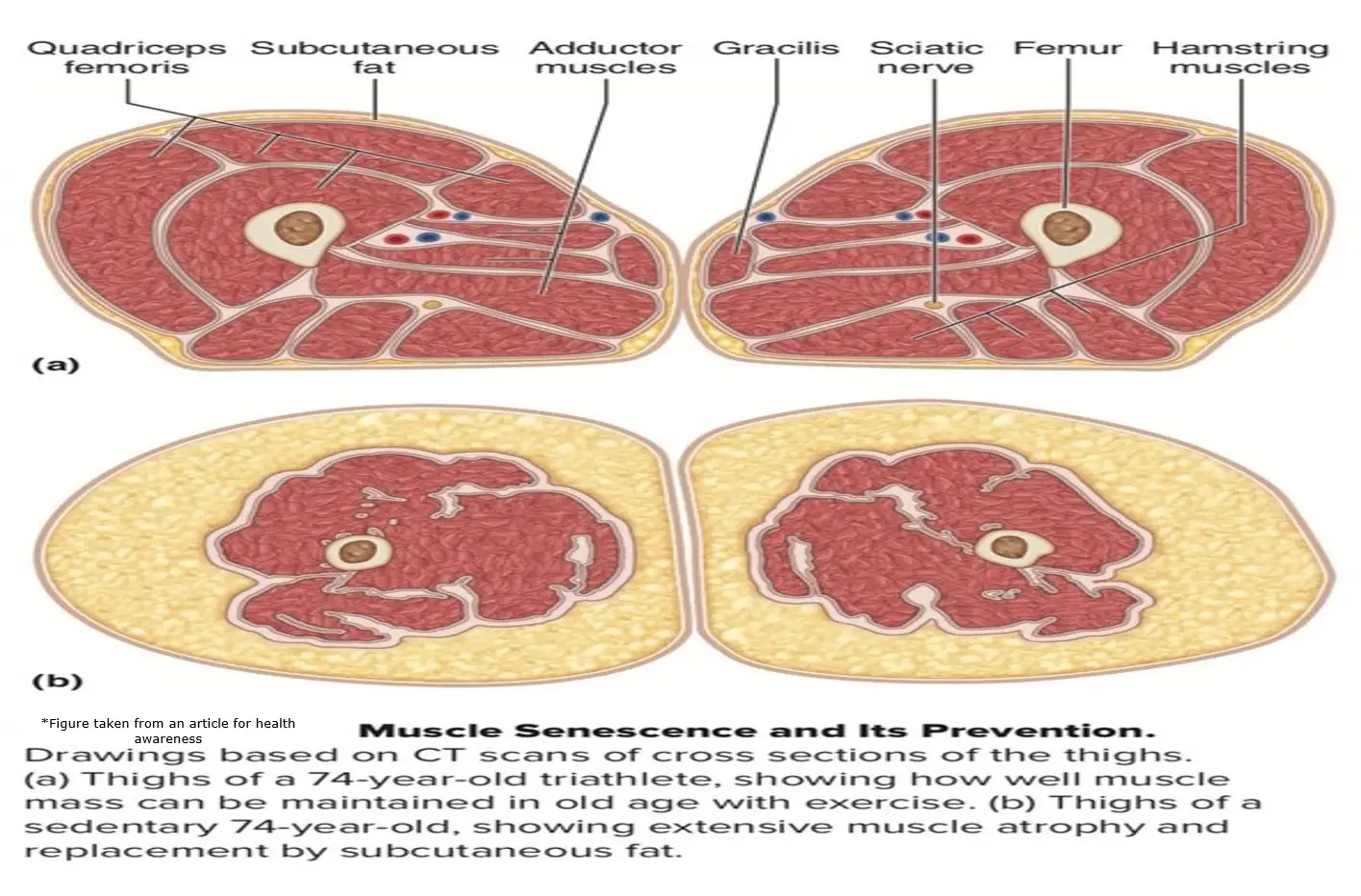
The Bone-on-Bone Consequence: In the sedentary leg, the atrophied, fatty muscle cannot fire quickly or strongly enough to dampen the load. The result? The shock bypasses the muscle and hammers directly into the articular cartilage and subchondral bone.
Over years, this unbuffered impact destroys the joint. Weak muscles do not just accompany arthritis; they precede and cause it.
The "Junk" in the System: Vascular Compression and Pain
In the sedentary scan, I noted that the arteries and veins were obscured by fatty tissue. This is a critical point that is rarely discussed.
Healthy muscle acts as a peripheral heart. When strong muscles contract, they pump venous blood and lymph back to the heart. This is the "muscle pump" mechanism. When muscle is replaced by static, non-contractile fat, this pump fails. Fluid accumulates (edema), metabolic waste products settle in the tissues, and oxygen delivery to the nerves is compromised.
This leads to a hypoxic (low oxygen) environment in the tissues, which is a primary trigger for chronic, nagging pain that patients cannot pinpoint but feel constantly.